- Record: found
- Abstract: found
- Article: not found
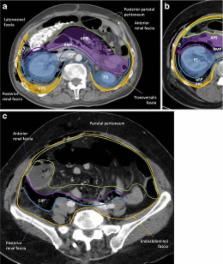
The anatomical compartments and their connections as demonstrated by ectopic air
Read this article at

Abstract
Air/gas outside the aero-digestive tract is abnormal; depending on its location, it is usually called emphysema, referring to trapped air/gas in tissues, or ectopic air/gas. It can be associated to a wide range of disorders, and although it usually is an innocuous condition, it should prompt a search for the underlying aetiology, since some of its causes impose an urgent treatment. In rare instances, it may itself represent a life-threatening condition, depending on the site involved and how quickly it evolves. Abnormal air/gas beyond viscera and serosal spaces, reaches its location following some anatomic boundaries, such as fascia, which may help search the source; however if the air pressure exceeds the strength of the tissues, or the time between the aggression and the imaging is too long, the air/gas is almost everywhere, which may hinder its cause. Good knowledge of the anatomic spaces and how they connect between them facilitates the quick detection of the cause.
Teaching points
• Ectopic air can be depicted on conventional radiographs; but CT is more sensitive and accurate
• Visceral and retropharyngeal spaces directly communicate with mediastinum
• Renal fascia is a single multilaminated structure, which contains potential space
Related collections
Most cited references32
- Record: found
- Abstract: found
- Article: not found
Subcutaneous and mediastinal emphysema. Pathophysiology, diagnosis, and management.
- Record: found
- Abstract: found
- Article: not found
Emphysematous infections of the abdomen and pelvis: a pictorial review.
- Record: found
- Abstract: found
- Article: not found