- Record: found
- Abstract: found
- Article: found
Changes in breast cancer grade from biopsy to excision following surgery or primary chemotherapy
Read this article at
Summary
Objective
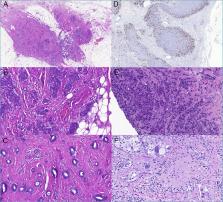
To compare histological grade (G) of breast cancer and its components (scores for tubule formation - T, nuclear pleomorphism - P and mitotic counts - M) in core needle biopsies (CNBs) and surgical excision specimens (EXC) in patients treated with primary surgery (CHIR) or primary chemotherapy (PST).
Methods
Grade of matched pairs of carcinomas in CNB and EXC was assessed according to the Nottingham grading system.
Results
PST cases tended to have higher pretreatment G. Concordance rates in the CHIR (n = 760) and PST (n = 148) groups for T, P, M and G were 79%, 70%, 75%, 71% and 77%, 70%, 50%, 62%, respectively; differences in concordance rates were significant in M (p < 0.0001) and G (p = 0.024). For discordant cases in the CHIR group, CNBs tended to overestimate T and underestimate P, M and G, whereas in the PST group, the same trends were identified for T and P, but there was a significant tendency for M and G to be lower in EXC specimens.
Related collections
Most cited references26
- Record: found
- Abstract: found
- Article: not found
pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: experience from a large study with long-term follow-up
- Record: found
- Abstract: found
- Article: not found
Pathological prognostic factors in breast cancer. II. Histological type. Relationship with survival in a large study with long-term follow-up.
- Record: found
- Abstract: found
- Article: not found