- Record: found
- Abstract: found
- Article: found
Impact of the COVID-19 pandemic on anxiety and depression symptoms of young people in the global south: evidence from a four-country cohort study
Read this article at
Abstract
Objective
To provide evidence on the effect of the COVID-19 pandemic on the mental health of young people who grew up in poverty in low/middle-income countries (LMICs).
Design
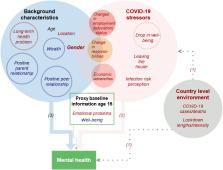
A phone survey administered between August and October 2020 to participants of a population-based longitudinal cohort study established in 2002 comprising two cohorts born in 1994–1995 and 2001–2002 in Ethiopia, India (Andhra Pradesh and Telangana), Peru and Vietnam. We use logistic regressions to examine associations between mental health and pandemic-related stressors, structural factors (gender, age), and lifelong protective/risk factors (parent and peer relationship, wealth, long-term health problems, past emotional problems, subjective well-being) measured at younger ages.
Setting
A geographically diverse, poverty-focused sample, also reaching those without mobile phones or internet access.
Participants
10 496 individuals were approached; 9730 participated. Overall, 8988 individuals were included in this study; 4610 (51%) men and 4378 (49%) women. Non-inclusion was due to non-location or missing data.
Main outcome measures
Symptoms consistent with at least mild anxiety or depression were measured by Generalized Anxiety Disorder-7 (≥5) or Patient Health Questionnaire-8 (≥5).
Results
Rates of symptoms of at least mild anxiety (depression) were highest in Peru at 41% (32%) (95% CI 38.63% to 43.12%; (29.49–33.74)), and lowest in Vietnam at 9% (9%) (95% CI 8.16% to 10.58%; (8.33–10.77)), mirroring COVID-19 mortality rates. Women were most affected in all countries except Ethiopia. Pandemic-related stressors such as health risks/expenses, economic adversity, food insecurity, and educational or employment disruption were risk factors for anxiety and depression, though showed varying levels of importance across countries. Prior parent/peer relationships were protective factors, while long-term health or emotional problems were risk factors.
Related collections
Most cited references70
- Record: found
- Abstract: found
- Article: not found
A brief measure for assessing generalized anxiety disorder: the GAD-7.
- Record: found
- Abstract: found
- Article: not found
Coefficient alpha and the internal structure of tests
- Record: found
- Abstract: found
- Article: not found