- Record: found
- Abstract: found
- Article: found
Establishing and Governing e-Mental Health Care in Australia: A Systematic Review of Challenges and A Call For Policy-Focussed Research
Abstract
Background
Growing evidence attests to the efficacy of e-mental health services. There is less evidence on how to facilitate the safe, effective, and sustainable implementation of these services.
Objective
We conducted a systematic review on e-mental health service use for depressive and anxiety disorders to inform policy development and identify policy-relevant gaps in the evidence base.
Methods
Following the PRISMA protocol, we identified research (1) conducted in Australia, (2) on e-mental health services, (3) for depressive or anxiety disorders, and (4) on e-mental health usage, such as barriers and facilitators to use. Databases searched included Cochrane, PubMed, PsycINFO, CINAHL, Embase, ProQuest Social Science, and Google Scholar. Sources were assessed according to area and level of policy relevance.
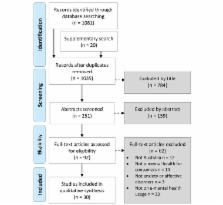
Results
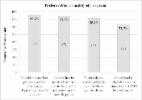
The search yielded 1081 studies; 30 studies were included for analysis. Most reported on self-selected samples and samples of online help-seekers. Studies indicate that e-mental health services are predominantly used by females, and those who are more educated and socioeconomically advantaged. Ethnicity was infrequently reported on. Studies examining consumer preferences found a preference for face-to-face therapy over e-therapies, but not an aversion to e-therapy. Content relevant to governance was predominantly related to the organizational dimensions of e-mental health services, followed by implications for community education. Financing and payment for e-services and governance of the information communication technology were least commonly discussed.
Conclusions
Little research focuses explicitly on policy development and implementation planning; most research provides an e-services perspective. Research is needed to provide community and policy-maker perspectives. General population studies of prospective treatment seekers that include ethnicity and socioeconomic status and quantify relative preferences for all treatment modalities are necessary.
Related collections
Most cited references48
- Record: found
- Abstract: not found
- Article: not found
Neurocognitive enhancement: what can we do and what should we do?
- Record: found
- Abstract: found
- Article: found
Extending an evidence hierarchy to include topics other than treatment: revising the Australian 'levels of evidence'
- Record: found
- Abstract: found
- Article: found