- Record: found
- Abstract: found
- Article: found
Analysis of risk factors in thoracic trauma patients with a comparison of a modern trauma centre: a mono-centre study
Read this article at
Abstract
Objectives
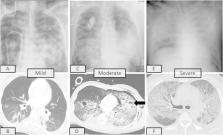
Thoracic trauma (TT) is the third most common cause of death after abdominal injury and head trauma in polytrauma patients. Its management is still a very challenging task. The purpose of this study was to analyse the risk factors affecting the outcome in a high-volume trauma centre and the efficacy of a specialised trauma team in level 1 trauma centres.
Patients and methods
Between January 2003 and December 2012, data of all patients admitted to the accident and emergency (A&E) department were prospectively collected at the German Trauma Registry (GTR) and thereafter retrospectively analysed.
Patients with chest trauma, an Injury Severity Score (ISS) ≥ 18 and an Abbreviated Injury Scale (AIS) > 2 in more than one body region were included. Patients were divided into two groups: group I included patients presenting with thoracic trauma between January 2003 and December 2007. The results of this group were compared with the results of another group (group II) in a later 5-year period (Jan. 2008–Dec. 2012). Univariate and multivariate analyses were performed, and differences with p < 0.05 were considered statistically significant.
Results
There were 630 patients (56%) with thoracic trauma. A total of 540 patients (48%) had associated extrathoracic injuries. Group I consisted of 285 patients (197 male, mean age 46 years). Group II consisted of 345 patients (251 male, mean age 49 years). Overall 90-day mortality was 17% ( n = 48) in group I vs. 9% ( n = 31) in group II ( p = 0.024). Complication rates were higher in group I ( p = 0.019). Higher Injury Severity Scores (ISSs) and higher Abbreviated Injury Acale (AIS) scores in the thoracic region yielded a higher rate of mortality ( p < 0.0001). Young patients (< 40 years) were frequently exposed to severe thoracic injury but showed lower mortality rates ( p = 0.014). Patients with severe lung contusions ( n = 94) (15%) had higher morbidity and mortality ( p < 0.001). Twenty-three (8%) patients underwent emergency thoracotomy in group I vs. 14 patients (4%) in group II ( p = 0.041). Organ replacement procedures were needed in 18% of patients in group I vs. 31% of patients in group II ( p = 0.038).
Conclusions
The presence of severe lung contusion, a higher ISS and AIS thoracic score and advanced age are independent risk factors that are directly related to a higher mortality rate. Management of blunt chest trauma with corrective chest tube insertion, optimal pain control and chest physiotherapy results in good outcomes in the majority of patients. Optimal management with better survival rates is achievable in specialised centres with multidisciplinary teamwork and the presence of thoracic surgical experience.
Related collections
Most cited references22
- Record: found
- Abstract: not found
- Article: not found
Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome). Use of the Bramson membrane lung.
- Record: found
- Abstract: found
- Article: not found
Appraisal of early evaluation of blunt chest trauma: development of a standardized scoring system for initial clinical decision making.
- Record: found
- Abstract: found
- Article: not found