- Record: found
- Abstract: found
- Article: found
Enhancing governance and health system accountability for people centered healthcare: an exploratory study of community scorecards in Afghanistan
Read this article at
Abstract
Background
The premise of patient-centered care is to empower patients to become active participants in their own care and receive health services focused on their individual needs and preferences. Afghanistan has evidenced enormous gains in coverage and utilization, but the quality of care remains suboptimal, as evidenced in the balanced scorecard (BSC) performance assessments. In the United States and throughout Africa and Asia, community scorecards (CSC) have proved effective in improving accountability and responsiveness of services. This study represents the first attempt to assess CSC feasibility in a fragile context (Afghanistan) through joint engagement of service providers and community members in the design of patient-centered services with the objective of assessing impact on service delivery and perceived quality of care.
Methods
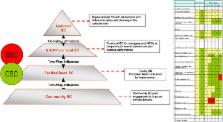
Six primary healthcare facilities were randomly selected in three provinces (Bamyan, Takhar and Nangarhar) and communities in their catchment area were selected for the study. Employing a multi-stakeholder strategy, community members and leaders, health councils, facility providers, NGO managers, and provincial directorates were engaged in a five-phase process to jointly identify structural and service delivery indicators (about 20), score performance and subsequently develop action plans for instituting improvements through participatory research methods. Three rounds of CSC assessments were conducted in each community. Over 470 community members, 34 health providers, and other provincial ministry staff participated in the performance audits.
Results
Structural capacity indicators including the number and cadre of service providers, particularly female providers, water and power supply, waiting rooms, essential medicines, and equipment scored low in the first round (30–50 %). Provider courtesy and quality of care received high scores (>90 %) throughout the study. Unrealistic community demands for ambulances and specialist doctors were mitigated by community education of entitlements described in the national standards for essential package of services. The joint interface meeting facilitated transparent dialogue between the community and providers and resulted in creative and participatory problem solving mechanisms and mobilization of resources.
Related collections
Most cited references30
- Record: found
- Abstract: found
- Article: not found
Neonatal and infant mortality in the ten years (1993 to 2003) of the Gadchiroli field trial: effect of home-based neonatal care.
- Record: found
- Abstract: found
- Article: not found
Global public health: a scorecard.
- Record: found
- Abstract: found
- Article: not found