- Record: found
- Abstract: found
- Article: found
Interpreting results, impacts and implications from WHO FCTC tobacco control investment cases in 21 low-income and middle-income countries
Read this article at
Abstract
Background
Tobacco control investment cases analyse the health and socioeconomic costs of tobacco use and the benefits that can be achieved from implementing measures outlined in the WHO Framework Convention on Tobacco Control (WHO FCTC). They are intended to provide policy-makers and other stakeholders with country-level evidence that is relevant, useful and responsive to national priorities and policy context.
Methods
This paper synthesises findings from investment cases conducted in Armenia, Cabo Verde, Cambodia, Chad, Colombia, Costa Rica, El Salvador, Eswatini, Georgia, Ghana, Jordan, Laos, Madagascar, Myanmar, Nepal, Samoa, Sierra Leone, Sri Lanka, Suriname, Tunisia and Zambia. We examine annual socioeconomic costs associated with tobacco use, focusing on smoking-related healthcare expenditures, the value of lives lost due to tobacco-related mortality and workplace productivity losses due to smoking. We explore potential benefits associated with WHO FCTC tobacco demand-reduction measures.
Results
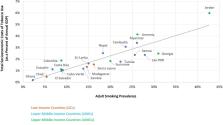
Tobacco use results in average annual socioeconomic losses of US$95 million, US$610 million and US$1.6 billion among the low-income (n=3), lower-middle-income (n=12) and upper-middle-income countries (n=6) included in this analysis, respectively. These losses are equal to 1.1%, 1.8% and 2.9% of average annual national gross domestic product, respectively. Implementation and enforcement of WHO FCTC tobacco demand-reduction measures would lead to reduced tobacco use, fewer tobacco-related deaths and reduced socioeconomic losses.
Related collections
Most cited references29
- Record: found
- Abstract: found
- Article: not found
Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study
- Record: found
- Abstract: found
- Article: not found
21st-Century Hazards of Smoking and Benefits of Cessation in the United States

- Record: found
- Abstract: found
- Article: found