- Record: found
- Abstract: found
- Article: found
Toward designing human intervention studies to prevent osteoarthritis after knee injury: A report from an interdisciplinary OARSI 2023 workshop
Read this article at
Abstract
Objective
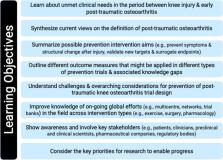
The global impact of osteoarthritis is growing. Currently no disease modifying osteoarthritis drugs/therapies exist, increasing the need for preventative strategies. Knee injuries have a high prevalence, distinct onset, and strong independent association with post-traumatic osteoarthritis (PTOA). Numerous groups are embarking upon research that will culminate in clinical trials to assess the effect of interventions to prevent knee PTOA despite challenges and lack of consensus about trial design in this population. Our objectives were to improve awareness of knee PTOA prevention trial design and discuss state-of-the art methods to address the unique opportunities and challenges of these studies.
Design
An international interdisciplinary group developed a workshop, hosted at the 2023 Osteoarthritis Research Society International Congress. Here we summarize the workshop content and outputs, with the goal of moving the field of PTOA prevention trial design forward.
Results
Workshop highlights included discussions about target population (considering risk, homogeneity, and possibility of modifying osteoarthritis outcome); target treatment (considering delivery, timing, feasibility and effectiveness); comparators (usual care, placebo), and primary symptomatic outcomes considering surrogates and the importance of knee function and symptoms other than pain to this population.
Conclusions
Opportunities to test multimodal PTOA prevention interventions across preclinical models and clinical trials exist. As improving symptomatic outcomes aligns with patient and regulator priorities, co-primary symptomatic (single or aggregate/multidimensional outcome considering function and symptoms beyond pain) and structural/physiological outcomes may be appropriate for these trials. To ensure PTOA prevention trials are relevant and acceptable to all stakeholders, future research should address critical knowledge gaps and challenges.
Related collections
Most cited references43
- Record: found
- Abstract: found
- Article: found
Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010
- Record: found
- Abstract: found
- Article: not found
Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact.
- Record: found
- Abstract: found
- Article: not found