- Record: found
- Abstract: found
- Article: found
Assessment of safety margin after microwave ablation of stage I NSCLC with three-dimensional reconstruction technique using CT imaging
Read this article at
Abstract
Objective
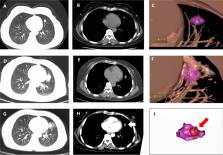
To assess the ablative margin of microwave ablation (MWA) for stage I non-small cell lung cancer (NSCLC) using a three-dimensional (3D) reconstruction technique.
Materials and methods
We retrospectively analyzed 36 patients with stage I NSCLC lesions undergoing MWA and analyzed the relationship between minimal ablative margin and the local tumor progression (LTP) interval, the distant metastasis interval and disease-free survival (DFS). The minimal ablative margin was measured using the fusion of 3D computed tomography reconstruction technique.
Results
Univariate and multivariate analyses indicated that tumor size (hazard ratio [HR] = 1.91, P < 0.01; HR = 2.41, P = 0.01) and minimal ablative margin (HR = 0.13, P < 0.01; HR = 0.11, P < 0.01) were independent prognostic factors for the LTP interval. Tumor size (HR = 1.96, P < 0.01; HR = 2.35, P < 0.01) and minimal ablative margin (HR = 0.17, P < 0.01; HR = 0.13, P < 0.01) were independent prognostic factors for DFS by univariate and multivariate analyses. In the group with a minimal ablative margin < 5 mm, the 1-year and 2-year local progression-free rates were 35.7% and 15.9%, respectively. The 1-year and 2-year distant metastasis-free rates were 75.6% and 75.6%, respectively; the 1-year and 2-year disease-free survival rates were 16.7% and 11.1%, respectively. In the group with a minimal ablative margin ≥ 5 mm, the 1-year and 2-year local progression-free rates were 88.9% and 69.4%, respectively. The 1-year and 2-year distant metastasis-free rates were 94.4% and 86.6%, respectively; the 1-year and 2-year disease-free survival rates were 88.9% and 63.7%, respectively. The feasibility of 3D quantitative analysis of the ablative margins after MWA for NSCLC has been validated.
Related collections
Most cited references32
- Record: found
- Abstract: found
- Article: not found
Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries
- Record: found
- Abstract: found
- Article: not found
Cancer statistics, 2019
- Record: found
- Abstract: found
- Article: not found