- Record: found
- Abstract: found
- Article: found
Overdiagnosing of femoroacetabular impingement: correlation between clinical presentation and computed tomography in symptomatic patients ☆ Translated title: Sobrediagnóstico do impacto femoroacetabular: correlação entre a clínica e a tomografia computadorizada em pacientes sintomáticos
Read this article at
Abstract
Objective
To correlate the angles between the acetabulum and the proximal femur in symptomatic patients with femoroacetabular impingement (FAI), using computed tomography (CT).
Methods
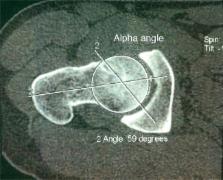
We retrospectively evaluated 103 hips from 103 patients, using multislice CT to measure the acetabular age, acetabular version (in its supraequatorial portion and in its middle third), femoral neck version, cervical-diaphyseal and alpha angles and the acetabular depth. For the statistical analysis, we used the Pearson correlation coefficient.
Results
There were inverse correlations between the following angles: (1) acetabular coverage versus alpha angle ( p = 0.019); (2) acetabular version (supraequatorial) versus alpha angle ( p = 0.049). For patients with femoral anteversion lower than 15 degrees: (1) acetabular version (supraequatorial) versus alpha angle ( p = 0.026); (2) acetabular version (middle third) versus alpha angle ( p = 0.02). For patients with acetabular version (supraequatorial) lower than 10 degrees: (1) acetabular version (supraequatorial) versus alpha angle ( p = 0.004); (2) acetabular version (middle third) versus alpha angle ( p = 0.009).
Conclusion
There was a statistically significant inverse correlation between the acetabular version and alpha angles (the smaller the acetabular anteversion angle was, the larger the alpha angle was) in symptomatic patients, thus supporting the hypothesis that FAI occurs when cam and pincer findings due to acetabular retroversion are seen simultaneously, and that the latter alone does not cause FAI, which leads to overdiagnosis in these cases.
Resumo
Correlacionar, por tomografia computadorizada (TC), os ângulos entre o acetábulo e o fêmur proximal em pacientes sintomáticos com impacto femoroacetabular (IFA).
Avaliamos, retrospectivamente, 103 quadris (103 pacientes) e medimos por TC multislice os ângulos de cobertura acetabular, de versão acetabular (em sua porção supraequatorial e no seu terço médio), de versão do colo femoral, cervicodiafisário, alfa e de profundidade acetabular. Para análise estatística, usamos o coeficiente de correlação de Pearson.
Houve correlação inversa entre os ângulos: 1) cobertura acetabular versus ângulo alfa (p = 0,019); 2) versão acetabular (supraequatorial) versus ângulo alfa (p = 0,049). Para pacientes com anteversão femoral menor do que 15°: 1) versão acetabular (supraequatorial) versus ângulo alfa (p = 0,026); 2) versão acetabular (terço médio) versus ângulo alfa (p = 0,02). Para pacientes com versão acetabular (supraequatorial) menor do que 10°: 1) versão acetabular (supraequatorial) versus ângulo alfa (p = 0,004); 2) versão acetabular (terço médio) versus ângulo alfa (p = 0,009).
Há correlação inversa estatisticamente significativa entre os ângulos de versão acetabular e o ângulo alfa (quanto menor o ângulo de anteversão acetabular, maior o ângulo alfa femoral) em pacientes sintomáticos. Isso reforça a hipótese de que o IFA ocorre quando há simultaneamente os achados de cam e pincer por retroversão acetabular e que esse não causa o IFA isoladamente, o que leva a sobrediagnóstico nesses casos.
Related collections
Most cited references60
- Record: found
- Abstract: found
- Article: not found
Femoroacetabular impingement: a cause for osteoarthritis of the hip.
- Record: found
- Abstract: found
- Article: not found
Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip.
- Record: found
- Abstract: found
- Article: not found