- Record: found
- Abstract: found
- Article: found
Evidences for a protective role of vitamin D in COVID-19
editorial
28 December 2020
Read this article at
There is no author summary for this article yet. Authors can add summaries to their articles on ScienceOpen to make them more accessible to a non-specialist audience.
Abstract
Introduction
Vitamin D and COVID-19
A growing number of concordant reports support a protective role for vitamin D in
reducing at least the risk/severity of respiratory tract infections (RTIs), especially
in the influenza and COVID-19 context.1–5
Major clinical reports show that vitamin D deficiency contribute to acute respiratory
distress syndrome (ARDS) SARS-CoV-2 and that case-fatality rates increase with age
and the highest SARS-CoV-2 serum concentrations.6 7
In addition, the outbreak of COVID-19 seems to occur mainly in the cold winter time,
when serum 25-hydroxyvitamin D (25(OH)D—calcidiol or calcifediol) concentrations are
the lowest, as well as the ultraviolet B (UVB) doses, whereas the number of cases
in the Southern Hemisphere near the end of summer are lower.8-
Targeted 25(OH)D serum concentration measurements and vitamin D supplementation is
strongly suggested have important patient and public health benefits.9 The positive
role of vitamin D replacement therapy (vDRT) in reducing risk and severity in COVID-19
patients is supported by several clinical evidences and RCTs are undergoing, however,
previous experiences of RCT related to vDRT are available from other lung viral infection
studies and even in mechanically ventilated adult intensive care unit (ICU) patients.10–14
These important observations are corroborated by several biological/molecular mechanisms
through vitamin D can generally reduce risk of infections and downregulate the immune/inflammatory
reaction. Indeed, functional vitamin D receptors (VDR) are highly-expressed in B-lymphocytes
and T-lymphocytes and mainly in monocytes/macrophages, justifying a role in modulating
both innate and adaptive immune responses15–18 (figure 1).
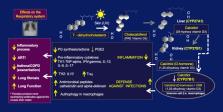
Figure 1
Proposed mechanism whereby 1,25(OH) D -VDR (D-hormone) signalling acts on the respiratory
system during the COVID-19 infection. 1,25(OH) D, 1,25-hydroxyvitamin D; ARTI, acute
respiratory tract infection; IFN-gamma, inteferon gamma; IL-6, inteleukin 6; IL10,
interleukin; IL -12, interleukin 12; IL-17, interleukin 17; Treg, T regulatory cells;
TNF, tumour necrosis factor; UV, ultraviolet; VDR, vitamin D receptor.
We will analyse and discuss such available clinical evidences on the light of vitamin
D molecular actions and the need to supplementation in COVID-19 patients.
Vitamin D is a steroidal hormone (D hormone) and may influence the immune response
in COVID-19
Vitamin D enters the body through dietary consumption (about 20% of vitamin D3) or
is synthesised by the skin (80%) from 7-dihydro-cholesterol (provitamin D or chlecalciferol)
after exposure to type B ultraviolet (UVB) which varies seasonally (figure 1).
The discovered presence of the VDR in activated T cells and monocytes, first suggested
in 1983 that vitamin D may have a role in the function of the immune system.19
As matter of fact, vitamin D has received increased worldwide attention for its involvement
in reducing risk for several chronic diseases, besides infectious diseases, including
type 1 diabetes and notably autoimmune rheumatic diseases for the reason that may
interfere with the immune system.20
The biological/molecular evidence for the interactions of vitamin D with the immune
response is that its final active metabolite, namely calcitriol (1,25(OH)2D3), due
to its structural origin from cholesterol, is molecularly considered a steroid hormone
(D-hormone) like others (ie, sex hormones, cortisol) and analogously to glucocorticoids
(and sex hormones) can exerts immunomodulatory/antinflammatory activities through
functional cell steroid receptors21–23 (figure 1).
Furthermore, the intensity and quality of the host immune/inflammatory response seems
to influence the clinical severity and mortality risk associated with viral diseases
(such as influenza and COVID-19) rather than the viral pathogen itself.24 25
Consequently, it is biologically plausible that 1,25(OH)2D3 may exert immunomodulatory
effects also in COVID-19 patients, playing a role in the regulation of both innate
and adaptive immunity.26
The intracellular conversion of 25(OH)D (calcidiol or calcifediol) into the active
metabolite 1,25(OH)2D3, (calcitriol), through the intracrine actions of the enzyme
1-alpha-hydroxylase (CYP27B1), is distinct from the 1,25(OH)2D3 produced in kidneys
and released into the systemic circulation; however, both have autocrine and paracrine
functions that enhance host immunity, for example, by upregulating the antimicrobial
peptides cathelicidin and alpha-defensin26 (figure 1).
In addition, the lung epithelium also expresses the VDR and CYP27B1 and may be an
important target tissue for the vitamin D endocrine system.27
Innate immunity is the first line of defence against bacteria and viruses and is activated
within hours of exposure to the pathogen.
Calcitriol (1,25(OH)2D3) can inhibit inflammatory T cell cytokines such as interleukin
(IL)-2 and IL-17 and toll-like receptors present on monocytes28 29 (figure 1).
On the other hands, in response to calcitriol administration, Th cells in an inflammatory
environment they exhibit an enhanced potential for Th2 polarisation along with a decreased
potential for Th17 polarisation.30
High doses of calcitriol supplementation in healthy human subjects (1 µg two times
per day for 7 days) leads to a dramatic reduction in the levels of proinflammatory
cytokine IL-6, secreted by peripheral mononuclear cells.31
All these effects likely combine and translate in the induction of potential regulatory
T cells, which are important for regulating immune responses and for the development
of autoreactivity32 (figure 1).
Adaptive immunity is the immune process by which immunological memory to a specific
antigen is established and requires a timeline much slower than innate immunity. Adaptive
immunity is further mediated through two types of lymphocytic cells: T cells for cell-mediated
immunity and B cells that are responsible for humoral immunity. Activated B cells
produce specific antibodies to the pathogen and neutralise or destroy it through a
variety of mechanisms.
Calcitriol has been shown to suppress adaptive immunity in animal models, however,
recent data are not yet sufficient to prove a real role for vitamin D in the modulation
of adaptive immune system in humans,33
Lastly, the ‘cytokine storm’ is a term used to describe a hyperactive immune response
to COVID-19. Although much yet to learnt about the pathophysiology of ‘cytokine storm’,
it is considered to be mediated by the activation of the innate immune system and
with an overly increased activation of the adaptive immunity.34 35
The clinical manifestations of this acute reaction include critical lung injury, wide-spread
tissue damage, multiorgan failure and frequently death.
Regarding vitamin D and gender, it is known that mortality is higher in COVID-19 male
than female patients, possibly because, due to androgens, the adaptive immune response
in men is less efficient to mount an antibody response (against SARS-CoV-2), with
the result that their disease further evolves severely36 (figure 1).
On the contrary, female COVID-19 patients react immunologically better due to enhancing
estrogenic effects on adaptive immunity, with the result to produce specific antibodies
that may neutralise earlier the virus, like what happen with other infections and
after vaccinations.37
Interestingly, it has been reported that in severe COVID-19 patients, the average
of SARS- CoV-2 IgG antibody serum concentrations in women tended to be higher and
the generation of IgG antibody was stronger in female than male patients.38
Therefore, vitamin D deficiency, seems to add further risks to the male COVID-19 patients,
in fact concentrations of 25(OH)D, have been found significantly lower only in male
patients COVID-19 vs women and controls (p=0.0006) and were not confounded by vitamin
D-impacted comorbidities and seasonality. Conclusion, vitamin D deficiency seems a
prevalent and further risk factor for severe COVID-19 male patients.39
Vitamin D and RTIs: lesson from the recent experience
The seasonality of viral RTIs such as those caused by influenza virus and rhinovirus
has been recognised from long time and is even considered to be one of the major contributor
to seasonal variations in human mortality.40
As matter of fact, a recent large study found that sunlight UV radiation dose is negatively
correlated with the percent positive patients for SARS-CoV-2 and for four other common
human coronaviruses in the USA, and this association is season-related with lowest
vitamin D serum concentrations.41
In a large population survey (6789 participants), the prevalence of RTIs and altered
lung function showed a strong seasonal pattern and linear association in the opposite
direction to the vitamin D serum concentrations.42
A more detailed study evaluating the link between vitamin D concentrations and ARDS,
patients with 25(OH)D3 <20 ng/mL showed a significantly higher odds of ARDS compared
with patients with 25(OH)D >20 ng/mL after adjustment for age, gender, diagnostic
category, staging and degree of cigarette consumption, (p=0.032).7
Interestingly, when 25(OH)D concentrations were analysed with logistic regression
as a continuous exposure in 0.4 ng/mL increments, the odds of ARDS decreased by 17%
for every 0.4 ng/mL increase in 25(OH)D (OR 0.83 (95% CI 0.69 to 0.98; p=0.033).7
In another study, it was found that each 4 ng/mL increase in 25(OH)D was associated
with a 7% lower risk of lung infection (95 % CI 3% to 11 %) after adjustment for lifestyle,
socioeconomic factors and adiposity.42
Therefore, it has been argued that vitamin D status should be taken into account as
an important contributor in determining the population susceptibility to seasonal
epidemic outbreaks, together with the effects of augmented indoor confinement in wintertime
(ie, school) and increased circulating reservoirs of respiratory viruses.43
Furthermore, another large observational study evaluating healthy adults during the
fall and winter of 2009–2010, investigated the relationship between serum 25(OH)D
concentrations and incidence of acute RTIs (ARTIs).44
The result was that only 17% of patients showing serum 25(OH)D concentrations over
38 ng/mL throughout the study developed ARTIs, on the contrary 45% of those with serum
concentrations less than 38 ng/mL did.
Concentrations of vitamin D over 40 ng/mL induced a significant (p<0.0001) twofold
reduction in risk of developing ARTIs including a strong reduction in the percentage
of days of illness (figure 1).
The negative correlation between seasonality (winter) of inflammatory conditions (ie,
rheumatoid arthritis) and vitamin D concentrations (UV effects) has been already deeply
analysed and it links the immune response with the 25(OH)D concentrations.45 46
More recently, the prevalence of vitamin D insufficiency and deficiency, (serum concentrations
of 12–20 and <12 ng/mL, respectively), was assessed in association with mortality
from respiratory diseases during 15 years of follow-up in a cohort of 9548 adults,
aged 50–75 years.47
Overall, 41% of respiratory disease mortality was statistically attributable to vitamin
D insufficiency or deficiency.
Previously, in a systematic review and meta-analysis, 25 randomised, double blind,
placebo controlled trials (total 11 321 participants, aged 0–95 years) were selected
in order to evaluate if supplementation of vitamin D might reduce the risk of ARTIs.48
Interestingly, vitamin D supplementation reduced significantly the risk of ARTI among
all participants (p<0.001) and in a subgroup analysis, protective effects against
ARTIs were observed in those individuals receiving daily or weekly vitamin D without
additional bolus doses, but not in those receiving one or more bolus doses (p=0.05).
Among those receiving daily or weekly vitamin D, protective effects were stronger
in those with baseline 25(OH)D <10 ng/mL than in those with baseline 25(OH)D levels
≥10 ng/mL (for interaction p=0.006). The lesson from these recent evidences seem to
confirm that vitamin D supplementation is safe and might protect at least against
ARTIs overall.49
This experience seems today replicated in COVID-19 patients.
Clinical evidences for vitamin D involvement in COVID-19 and earliest therapeutical
interventions
SARS-CoV-2 is the major allmark of COVID-19, with clinical outcomes ranging from mild
to severe, including death.
The most recent evidences support the clinical experience that vitamin D supplementation
would be advantageous in the treatment of COVID-19 patients, in reducing the presence
of SARS-CoV-2 at the level of the upper respiratory tract, in making the patients
less infectious (justifying the presence of negative PCR in people with higher 25(OH)D)
and in preventing a more severe symptomatology.2
On the other hands, a very recent study, showed the first direct evidence of the association
between vitamin D deficiency and potentially insufficient treatment with testing positive
for COVID-19.50
The multivariable analysis suggested that individuals with most recent vitamin D deficiency
whose treatments were not increased (remained vitamin D deficient), were at higher
risk of testing positive for COVID-19, than were individuals with serum concentrations
that were likely to be sufficient confirming the majority of reports.51
In addition, a very recent small study showed that 84.6% of intensive treatment unit
(ITU) severe COVID-19 patients had deficiency of vitamin D (<12 ng/mL) compared with
only 57.1% of patients on medical ward.51
Similar results were confirmed in another study in which serum 25(OH)D concentrations
were evaluated in 134 inpatients with positive SARS-CoV-2 swab or clinic-radiological
diagnosis of COVID-19.2 Again, ITU COVID-19 patients showed lower 25(OH)D serum concentrations
compared with non-ITU patients despite being younger, (13.4 ng/mL±6.7 vs. non-ITU:
19.4 ng/mL±15.3;p=0.03).
Nevertheless, ITU COVID-19 patients showed a significantly higher prevalence of vitamin
D deficiency, with only 19% being vitamin D replete compared with 39.1% of non-ITU
patients (p=0.02). However, serum 25(OH)D concentrations were not associated with
mortality (p=0.94) probably due to the short time of observation.
These results suggest the acute and follow-up assessment of serum 25(OH)D concentrations
during COVID-19 admission.
Another study, among patients with vitamin D deficiency, further confirmed higher
incidence of noninvasive ventilation support and high-dependency unit admission (p=0.042),
with older COVID-19 adults demonstrating worse morbidity outcomes. Again the vitamin
D status may be considered at least an useful prognosticator.52
A number of investigations confirm that deficient/insufficient concentrations of vitamin
D are associated with the hospitalisation of COVID-19 patients, and less than 16 ng/mL
values of the serum vitamin D have been reported to be possibly associated even with
increased risk of sepsis in critically ill patients.53 54
A large Israeli studied cohort, proved that, low serum 25(OH)D concentrations almost
doubled the risk for hospitalisation due to the COVID-19 infection.55
Finally, in a very recent case–control study, the serum 25(OH)D concentration in COVID-19
patient was found the lowest in severe/criticalcases, compared with mild cases. Severe/critical
COVID-19 cases were significantly older and had higher percentages of comorbidity
(renal failure) compared with mild cases, however, the statistically significant associations
remained even after controlling for demographics and comorbidities.56
Of course, the majority of these studies has aimed to correct the results from concomitant
risk factors for vitamin D deficiency, but a residual confounding is still always
possible. In fact, factors associated with worse COVID-19 prognosis include old age,
ethnicity, male sex, socioeconomic level, as well as comorbidities like obesity, diabetes
and hypertension, and all of these also associate with deficiency of vitamin D.57
Therefore, the absence of specific treatment for COVID-19 generated many trials, but
so far without final guide lines, the same holds true for testing the potential benefits
of vitamin D supplementation of patients with SARS-CoV-2 infections.58
Interesting a pilot RCT published in October 2020, demonstrated that administration
of a high dose of Calcifediol (25(OH)D), significantly reduced the need for ICU treatment
of patients requiring hospitalisation due to proven COVID-19.59
At the same time, in a clinical cases series report, COVID-19 patients who received
a high dose of vitamin D supplementation, they achieved normalisation of vitamin D
serum concentrations and improved clinical recovery, evidenced by decrease in inflammatory
biomarker status, lower oxygen requirements and finally less days of hospitalisation.60
In addition, it has been already published a pragmatic trial design that will allow
parallel testing of vitamin D3 supplementation for early treatment and postexposure
prophylaxis of COVID- 19.61
To conclude, according to National Institute of Health (NIH) Trialnet database, several
observational and intervention studies, including some RCT, are running and should
provide guidelines within a few months.62 63
In essence, the rationale for intervention studies with vitamin D in cOVID-19 patients,
isfocused on the ability of 1,25(OH)2D3 to activate the native immune defence system,
while reducing the proinflammatory cytokine production and tapering down the acquired
immune system.64
In addition, as discussed previously in this text, vitamin D deficiency may predispose
to increased risk of infections including SARS-CoV-2, and its supplementation may
decrease the risk of upper respiratory infections.
How to supplement vitamin D in COVID-19 patients with deficiency
Although the degree of protection generally increases as 25(OH)D serum concentration
increases, the optimal range is considered to be in the range of 40–60 ng/mL (100–150 nmol/L).
In order achieve those levels, approximately half the population should take at least
2000–5000 IU/day of vitamin D.65
The supplementation with calcidiol (25(OH)D) may present some advantages over the
native vitamin D (cholecalciferol), in fact, calcidiol has a more reliable intestinal
absorption (close to 100%) and its administration can rapidly restore serum concentrations
of 25OHD as it does not require hepatic 25-hydroxylation (CYP27A1) (figure 1).
This is especially relevant in clinical situations whereby rapid restoration of serum
25OHD is desirable and expression is compromised. Such impaired hepatic vitamin D
hydroxylation by cytochrome p450 2R1 (CYP2R1) activity has been well demonstrated
in several animal models of obesity, diabetes or glucocorticoid excess and in patients
with COPD or asthma.66
Various loading doses have been studied for achieving a 25(OH)D concentration of 30 ng/mL.
For example, one study used a weekly or fortnightly dose totaling 100 000–2 00 000 IU
over 8 weeks (1800 or 3600 IU/day).67
Clinical data suggest that daily or weekly doses offer better results than bolus in
the protection against acute pulmonary infections and supplementation with extremely
high doses of vitamin D could be harmful and toxic, especially to elderly individuals.68
69
Some reports just speculated on single high vitamin D doses and mechanisms for prevention
and treatment of COVID-19 patients.70
Therefore, the supplementation of vitamin D by bolus or extremely high doses (ie,
600 000 UI single dose oral dose) should be avoided since can increase the risk of
intoxication without evidence of benefits at least in COVID-19 patients.65
In addition, from the literature, for healthy individuals, it is suggested taking
10 000 IU/day for a month, which is effective in rapidly increasing serum concentrations
of 25(OH)D into the optimal range of 40–60 ng/mL.10
To maintain that level after that first month, the dose can be decreased to almost
2000–3000 IU/day.
However, measuring serum 25(OH)D concentration would be useful to determine baseline
and the achieved 25(OH)D concentrations.
Patients hospitalised with COVID-19 should have baseline serum 25(OH)D concentrations
measured and must be supplemented at least to a level ≥30 ng/mL (optimal 40–60), especially
when the baseline level is <10 ng/mL and such deficiency is significantly more present
in male patients.71
In conclusion, we might suggest in COVID-19 patients with 25(OH)D serum levels under
20 ng/mL that the usual recommended dose for correction of deficiency should be 6000–7000
oral IU/day for the first 6–8 weeks. For maintenance, the dose should varies from
2000 to 3000 oral IU/day depending on the age and clinical condition of the patient
up to achieve the suggested concentrations.72
Conclusions
Given the evidence supporting the role of vitamin D in modulating immune function,
and the impact of vitamin D supplementation on vitamin D-deficient patients with COVID-19,
as well as the favourable safety profile (and low cost) of vitamin D, practical recommendations
should be synthesised as follows:
Current public health guidelines for optimising vitamin D status should be followed
always and clinical data from systematic reviews and meta-analyses show benefits in
the prevention of respiratory infections and improvement of pulmonary function when
vitamin D-deficient patients are supplemented.
The optimal vitamin D status of the host may contribute key immunoregulatory functions
in settings of viral respiratory infection and overall the altered immune-inflammatory
COVID-19 reactivity at least by downregulating overly exuberant cytokine responses
(pathological cytokine storm, in fact higher vitamin D levels correlate with lower
IL-6 levels).
Patients hospitalised with COVID-19 should have baseline serum 25(OH)D concentrations
measured and should be supplemented to a level >30 ng/mL (optimal 40–60 ng/mL), especially
when the baseline level is <10 ng/mL.
In COVID-19 patients with 25(OH)D serum concentrations under 20 ng/mL the recommended
dose for correction of deficiency is 6000–7000 oral IU/day for 6–8 weeks. For maintenance,
the dose varies from 2000 to 3000 oral IU/day depending on the age and clinical condition
of the individual up to reach optimal concentrations.
When it is not possible to measure baseline 25(OH)D concentrations in COVID-19 patients,
it seems essential supplementing with 2000–3000 oral IU per day up to the suggested
optimal serum concentrations (40–60 ng/mL).
A final message based on all the practical issues discussed: keep the vitamin D serum
concentrations during all the year between 40 and 60 ng/mL (100–150 nmol/L), it is
one of the fundamental care to reduce, at least the risk of RTIs, COVID-19 included.
Related collections
Most cited references68
- Record: found
- Abstract: found
- Article: found
Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths
William Grant, Henry Lahore, Sharon McDonnell … (2020)
- Record: found
- Abstract: found
- Article: found
The COVID-19 Cytokine Storm; What We Know So Far
Dina Ragab, Haitham Salah Eldin, Mohamed Taeimah … (2020)

- Record: found
- Abstract: found
- Article: found
Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data
Adrian Martineau, David A. Jolliffe, Richard Hooper … (2017)