- Record: found
- Abstract: found
- Article: found
Comparison of Laparoscopic and Microscopic Subinguinal Varicocelectomy in terms of Postoperative Scrotal Pain
Read this article at
Abstract
Laparoscopic varicocelectomy was found to be safe, effective, and minimally invasive. It appeared to result in less postoperative discomfort and earlier return to normal activity.
Abstract
Background and Objectives:
In this study, 2 different varicocelectomy methods were compared with regard to postoperative scrotal pain, length of operation, and complications.
Methods:
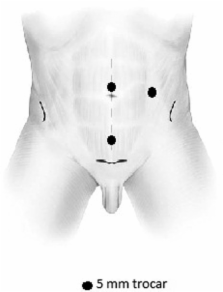
Forty varicocele patients, who visited our clinic because of infertility or scrotal pain between 2008 and 2009, were enrolled in this clinical study. Microscopic subinguinal varicocelectomy was performed on 20 patients in Group I, and laparoscopic varicocelectomy was performed on 20 patients in Group II. Following surgery, the patients were assessed for postoperative requirements for analgesia; return to normal activity; varicocele recurrence; hydrocele formation; scrotal pain at postoperative days 1, 3, and 7; and other complications.
Results:
Mean age was 24.2±3.4 years in Group I and 25.1±2.1 years in Group II. Mean pain scores at postoperative 1, 3, and 7 days in Group I were (5.20±1.14, 4.60±0.97, and 3.50±0.97, respectively) significantly higher than those of Group II (0.70±0.82, 0.60±0.84, and 0.10±0.32, respectively). Time to return to normal activity was significantly shorter in Group II (3.7±2.1 days) compared with Group I (6.8±3.4 days) (p=0.028). However, the number of recurrences and hydroceles, as a complication of varicocelectomy, was 2 times higher in Group II (10%) than in Group I (5%).
Related collections
Most cited references19
- Record: found
- Abstract: found
- Article: not found
Treatment of palpable varicocele in infertile men: a meta-analysis to define the best technique.
- Record: found
- Abstract: found
- Article: not found
Microsurgical inguinal varicocelectomy with delivery of the testis: an artery and lymphatic sparing technique.
- Record: found
- Abstract: found
- Article: not found