- Record: found
- Abstract: found
- Article: found
Association of Punitive and Reporting State Policies Related to Substance Use in Pregnancy With Rates of Neonatal Abstinence Syndrome
Read this article at
Abstract
This cross-sectional study examines the association of state-level punitive or reporting policies related to substance use during pregnancy with rates of neonatal abstinence syndrome.
Key Points
Question
Are state punitive or reporting policies related to substance use during pregnancy associated with rates of neonatal abstinence syndrome (NAS)?
Finding
In this repeated cross-sectional study of nearly 4.6 million births in 8 states, policies that criminalized substance use during pregnancy, considered it grounds for civil commitment, or considered it child abuse or neglect were associated with significantly greater rates of NAS in the first full year after enactment and more than 1 full year after enactment. Policies requiring reporting of suspected prenatal substance use were not associated with rates of NAS.
Abstract
Importance
Despite the rapidly changing policy environment regarding substance use during pregnancy, information is lacking on the association of state policies with neonatal abstinence syndrome (NAS).
Objective
To determine if punitive or reporting state policies related to substance use during pregnancy are associated with NAS rates.
Design, Setting, and Participants
This repeated cross-sectional study used retrospective, difference-in-difference analysis of live births in the State Inpatient Databases from 8 US states in varying years between January 1, 2003, and December 31, 2014. States without punitive or reporting policies were compared with states with policies before and after policy enactment using logistic regression models adjusted for individual and county-level factors and state and year fixed effects. Analyses were conducted from April 10, 2019, to July 30, 2019.
Exposures
Time since enactment of state policies related to substance use in pregnancy, county-level rurality and unemployment, and presence of specialized treatment programs for pregnant and postpartum women in a county.
Results
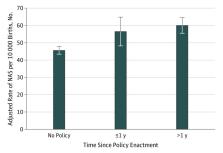
Among 4 567 963 live births, 23 377 neonates (0.5%) received a diagnosis of NAS. Among neonates with NAS, 3394 (14.5%) lived in counties without any treatment programs specifically for pregnant and postpartum women, 20 323 (86.9%) lived in metropolitan counties, and 8135 (34.8%) lived in counties in the highest unemployment quartile. In adjusted analyses among neonates in states with punitive policies, odds of NAS were significantly greater during the first full calendar year after enactment (adjusted odds ratio, 1.25; 95% CI, 1.06-1.46; P = .007) and more than 1 full year after enactment (adjusted odds ratio, 1.33; 95% CI, 1.17-1.51; P < .001). After regression adjustment, the annual NAS rate was 46 (95% CI, 43-48) neonates with NAS per 10 000 live births in states without punitive policies; 57 (95% CI, 48-65) neonates with NAS per 10 000 live births in states with punitive policies during the first full year after enactment; and 60 (95% CI, 56-65) neonates with NAS per 10 000 live births in states with punitive policies in effect for more than 1 full year. There was no association between reporting policies and odds of NAS.
Related collections
Most cited references34
- Record: found
- Abstract: found
- Article: not found
Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009.

- Record: found
- Abstract: found
- Article: found
Opioid Use Disorder Documented at Delivery Hospitalization — United States, 1999–2014

- Record: found
- Abstract: found
- Article: found