- Record: found
- Abstract: found
- Article: found
25-hydroxyvitamin D and parathyroid hormone in new onset sepsis: A prospective study in critically ill patients
Read this article at
Abstract
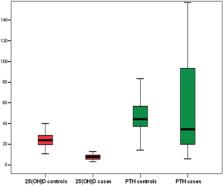
Hypovitaminosis D is highly prevalent in critically ill patients, and it has been suggested to be a risk factor for infections, sepsis and higher mortality. We sought to investigate whether serum 25-hydroxyvitamin D (25(OH)D) and parathyroid hormone (PTH) in critically ill patients with new onset sepsis are associated with severity and outcome. We prospectively included 50 consecutive critically ill adult cases with new onset sepsis and 50 healthy controls matched for age and sex. PTH and 25(OH)D were determined in serum via electrochemiluminescence immunoassays at inclusion in the study in all cases and controls, and one week after sepsis onset in cases. Patients had reduced 25(OH)D compared to controls at sepsis onset (7.9 ± 3 vs 24.6 ± 6.7 ng/mL, p < 0.001), whilst PTH was similar (median (range): 34.5 (5.7–218.5) vs 44.2 (14.2–98.1) pg/mL, p = 0.35). In patients, 25(OH)D upon enrollment and one week after did not differ significantly (7.9 ± 3 vs 7 ± 4.3 ng/mL, p = 0.19). All patients presented with hypovitaminosis D (25(OH)D < 20 ng/mL), while 40 patients (80 %) had vitamin D deficiency (25(OH)D < 12 ng/mL) at sepsis onset, including all ten (20 %) nonsurvivors, who died within 28 days from sepsis onset. Patients with sepsis (N = 28) and septic shock (N = 22) as well as survivors (N = 40) and nonsurvivors (N = 10) had similar 25(OH)D at enrollment (p > 0.05). 25(OH)D was positively correlated with ionized calcium (r = 0.46, p < 0.001) and negatively with PTH (p < 0.05), while inflammatory biomarkers or the severity scores exhibited no correlation with 25(OH)D. Patients with septic shock and nonsurvivors had lower PTH than patients with sepsis and survivors respectively (42.2 ± 42.9 vs 73.4 ± 61.9 pg/mL, p = 0.04, and 18.3 ± 10.7 vs 69.9 ± 58.8 pg/mL, p = 0.001, respectively). C-reactive protein was negatively associated with PTH (r = −0.44, p = 0.001). In conclusion, vitamin D deficiency was present in 80 % of critically ill patients at sepsis onset, while nonsurvivors exhibited lower PTH than survivors. Additional, larger and multicenter studies are warranted to elucidate the contribution of vitamin D and PTH to the pathogenesis of sepsis and its outcomes.
Highlights
Related collections
Most cited references51
- Record: found
- Abstract: found
- Article: found
The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).
- Record: found
- Abstract: found
- Article: found
Low plasma 25(OH) vitamin D level is associated with increased risk of COVID‐19 infection: an Israeli population‐based study
- Record: found
- Abstract: found
- Article: not found