- Record: found
- Abstract: found
- Article: found
Early Identification of CKD—A Scoping Review of the Global Populations

Read this article at
Abstract
Introduction
Decisions on whether to screen for chronic kidney disease (CKD) or not remain contentious in nephrology. This study provides a global overview of early CKD identification efforts.
Methods
Guidelines for scoping reviews were followed and studies were identified by searching MEDLINE, EMBASE, Cochrane Library, CINAHL, ISI Web of Science, and PsycINFO. Data extracted from included studies focused on the following 4 themes: study population, measurement methods, interventions used, and available policies.
Results
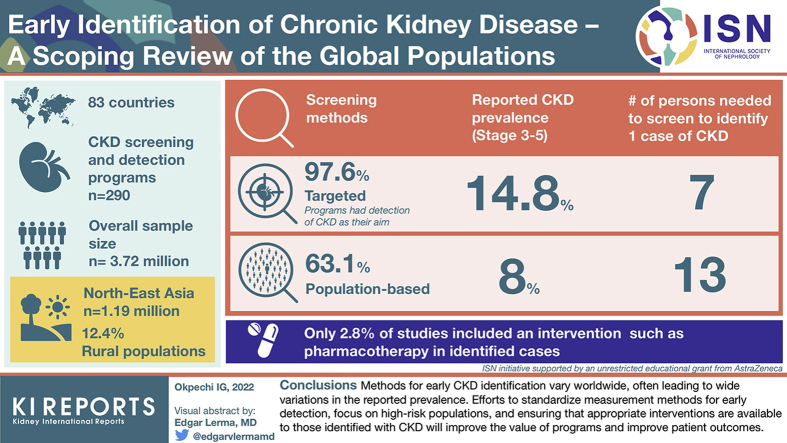
We identified 290 CKD screening and detection programs from 83 countries. Overall sample size was 3.72 million (North East Asia: 1.19 million), detection of CKD was the aim in 97.6%, 63.1% used population-based screening methods, and only 12.4% were in rural populations. Reported CKD prevalence (stages 3–5) was higher in targeted- (14.8%) than population-based studies (8.0%). Number of persons needed to screen (NNS) to identify 1 case was also lower in targeted studies (7 vs. 13). Single measurements (80%) and the combination of estimation of glomerular filtration rate with a urine test (albuminuria/proteinuria) (71.4%) were frequently used to detect CKD. Only 2.8% of studies included an intervention such as pharmacotherapy in identified cases. Policies on early identification were available in 30.1% of countries included.
Conclusion
Methods for early CKD identification vary worldwide, often leading to wide variations in the reported prevalence. Efforts to standardize measurement methods for early detection focusing on high-risk populations and ensuring appropriate interventions are available to those identified with CKD will improve the value of programs and improve patient outcomes.
Graphical abstract
Related collections
Most cited references50
- Record: found
- Abstract: found
- Article: not found
PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation

- Record: found
- Abstract: found
- Article: found