- Record: found
- Abstract: found
- Article: found
Risks and cancer associations of metachronous and synchronous multiple primary cancers: a 25-year retrospective study
Read this article at
Abstract
Background
The situation of patients developing multiple primary cancers is becoming more frequent and graver. This study investigated the risks of developing second primary cancers that are related to first primary cancers, and the interval times of synchronous and metachronous multiple primary cancers.
Patients and methods
Retrospective data were retrieved from 109,054 patients aged ≥18 who were diagnosed with a first solid cancer and registered at Siriraj Cancer Center between 1991 and 2015. A two-month period between first- and second- primary cancers was used to differentiate metachronous and synchronous multiple primary cancers. The combinations of subsequent cancers and relative risks (RRs) of having multiple primary cancers versus having single primary cancer for the top-ten first and second primary cancers were examined. The RR was adjusted for age of the first primary cancer. A survival analysis of the time to second-primary-cancer development was performed.
Results
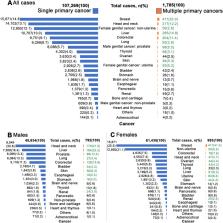
Multiple primary cancers were found in 1785 (1.63%) patients. Most (70.87%) second primary cancers occurred after 2 months of first breast, skin, colorectal, lung, head and neck, liver, male genital cancer–prostate, thyroid, and female genital cancer–non-uterine cancers, resulting in those cancers being classified as metachronous multiple primary cancer. After adjustment for age at first diagnosis, head and neck cancers had the highest metachronous association with second esophageal cancers (RR, 25.06; 95% CI, 13.41–50.77). Prostate cancer and second colorectal cancer also demonstrated a high metachronous association (RR, 2.00; 95% CI, 1.25–3.05). A strong synchronous association was found between uterine and ovarian cancers (RR, 27.77; 95% CI, 17.97–43.63). The median time from the first uterine cancer to second-cancer development was 55 days.
Conclusions
The top-ten most frequent multiple primary cancers were the following: breast; liver; head and neck; colorectal; male genital cancer–prostate; skin; female genital cancer–uterine; thyroid; lung; and female genital cancer–non-uterine. Second primary cancers showed specific associations that depended on the first primary cancer. Physicians should be cognizant of the most common combinations and the interval times of metachronous and synchronous multiple primary cancers.
Related collections
Most cited references35
- Record: found
- Abstract: found
- Article: not found
Cancer statistics, 2020

- Record: found
- Abstract: found
- Article: found
Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors
- Record: found
- Abstract: found
- Article: found