- Record: found
- Abstract: found
- Article: found
Impact of changes in head position during head and neck surgery on the depth of tracheal tube intubation in anesthetized children
Read this article at
Abstract
Background
The classic formula has been used to estimate the depth of tracheal tube intubation in children for decades. However, it is unclear whether this formula is applicable when the head and neck position changes intraoperatively.
Methods
We prospectively reviewed the data of 172 well-developed children aged 2–12 years (64.0% boys) who underwent head and neck surgery under general anesthesia. The distances from the tracheal carina to the endotracheal tube tip (CT), from the superior margin of the endotracheal tube tip to the vocal cord posterior commissure (CV), and from the tracheal carina to the posterior vocal commissure (TV) were measured in the sniffing position (maximum), neutral head, and maximal head flexion positions.
Results
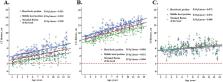
Average CT and CV in the neutral head position were 4.33 cm and 10.4 cm, respectively. They increased to 5.43 cm and 11.3 cm, respectively, in the sniffing position, and to 3.39 cm and 9.59 cm, respectively, in the maximal flexion position (all P-values < 0.001). TV remained unchanged and was only dependent on age. After stratifying patients by age, similar results were observed with other distances. CT and CV increased by 1.099 cm and 0.909 cm, respectively, when head position changed from neutral head to sniffing position, and decreased by 0.947 cm and 0.838 cm, respectively, when head position changed from neutral head to maximal flexion.
Related collections
Most cited references16
- Record: found
- Abstract: found
- Article: not found
[Height and weight standardized growth charts for Chinese children and adolescents aged 0 to 18 years].
- Record: found
- Abstract: found
- Article: not found
Appropriate placement of intubation depth marks in a new cuffed paediatric tracheal tube.
- Record: found
- Abstract: found
- Article: not found