- Record: found
- Abstract: found
- Article: found
Estimating age-specific COVID-19 fatality risk and time to death by comparing population diagnosis and death patterns: Australian data
Read this article at
Abstract
Background
Mortality is a key component of the natural history of COVID-19 infection. Surveillance data on COVID-19 deaths and case diagnoses are widely available in the public domain, but they are not used to model time to death because they typically do not link diagnosis and death at an individual level. This paper demonstrates that by comparing the unlinked patterns of new diagnoses and deaths over age and time, age-specific mortality and time to death may be estimated using a statistical method called deconvolution.
Methods
Age-specific data were analysed on 816 deaths among 6235 cases over age 50 years in Victoria, Australia, from the period January through December 2020. Deconvolution was applied assuming logistic dependence of case fatality risk (CFR) on age and a gamma time to death distribution. Non-parametric deconvolution analyses stratified into separate age groups were used to assess the model assumptions.
Results
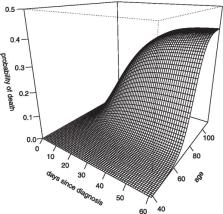
It was found that age-specific CFR rose from 2.9% at age 65 years (95% CI:2.2 – 3.5) to 40.0% at age 95 years (CI: 36.6 – 43.6). The estimated mean time between diagnosis and death was 18.1 days (CI: 16.9 – 19.3) and showed no evidence of varying by age (heterogeneity P = 0.97). The estimated 90% percentile of time to death was 33.3 days (CI: 30.4 – 36.3; heterogeneity P = 0.85). The final age-specific model provided a good fit to the observed age-stratified mortality patterns.
Conclusions
Deconvolution was demonstrated to be a powerful analysis method that could be applied to extensive data sources worldwide. Such analyses can inform transmission dynamics models and CFR assessment in emerging outbreaks. Based on these Australian data it is concluded that death from COVID-19 occurs within three weeks of diagnosis on average but takes five weeks in 10% of fatal cases. Fatality risk is negligible in the young but rises above 40% in the elderly, while time to death does not seem to vary by age.
Related collections
Most cited references26
- Record: found
- Abstract: found
- Article: not found
Estimates of the severity of coronavirus disease 2019: a model-based analysis

- Record: found
- Abstract: found
- Article: not found