- Record: found
- Abstract: found
- Article: found
Seventeen Cases of Primary Hyperparathyroidism in Pregnancy: A Call for Management Guidelines

Read this article at
Abstract
Context
The risks of primary hyperparathyroidism (pHPT) to pregnant women and their fetuses appear to increase commensurate with serum calcium levels. The management strategy for pHPT must be adapted in pregnancy and should reflect the severity of hypercalcemia. However, no guidelines exist to assist clinicians.
Methods
The experience of a high-volume multidisciplinary endocrine surgical service in treating a consecutive series of pregnant women with pHPT referred for parathyroidectomy is presented and data are compared with a nonpregnant cohort with pHPT. A review of pHPT and pregnancy outcomes in the literature is provided.
Results
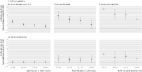
Seventeen pregnant women and 247 age range–matched nonpregnant women with pHPT were referred for surgery over 11 years. Mean serum calcium level was higher in the pregnant cohort (2.89 vs 2.78 mmol/L; P = 0.03). Preoperative localization with ultrasound succeeded in eight pregnant women (47%) and sestamibi scanning did in two of six (33% imaged preconception), compared with 84 (34%) and 102 (42%) control subjects, respectively (not significant). Parathyroidectomy was performed under general anesthesia between 12 and 28 weeks’ gestation with no adverse pregnancy outcomes resulting. Cure rate was 100% vs 96% in controls.
Conclusion
pHPT in pregnancy is a threat to mother and child. Medical management may be appropriate in mild disease, but in moderate to severe disease, parathyroidectomy under general anesthesia in the second trimester is safe. Localization using ionizing radiation/MRI is unnecessary, because surgical intervention in a high-volume multidisciplinary setting has excellent outcomes. Guidelines on the topic would assist clinicians.
Related collections
Most cited references56
- Record: found
- Abstract: found
- Article: found
Cardiovascular mortality after pre-eclampsia in one child mothers: prospective, population based cohort study
- Record: found
- Abstract: found
- Article: not found