- Record: found
- Abstract: found
- Article: found
Clinical Approach to Supranuclear Brainstem Saccadic Gaze Palsies
Read this article at
Abstract
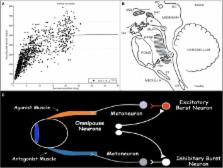
Failure of brainstem supranuclear centers for saccadic eye movements results in the clinical presence of a brainstem-mediated supranuclear saccadic gaze palsy (SGP), which is manifested as slowing of saccades with or without range of motion limitation of eye movements and as loss of quick phases of optokinetic nystagmus. Limitation in the range of motion of eye movements is typically worse with saccades than with smooth pursuit and is overcome with vestibular–ocular reflexive eye movements. The differential diagnosis of SGPs is broad, although acute-onset SGP is most often from brainstem infarction and chronic vertical SGP is most commonly caused by the neurodegenerative condition progressive supranuclear palsy. In this review, we discuss the brainstem anatomy and physiology of the brainstem saccade-generating network; we discuss the clinical features of SGPs, with an emphasis on insights from quantitative ocular motor recordings; and we consider the broad differential diagnosis of SGPs.
Related collections
Most cited references96
- Record: found
- Abstract: not found
- Article: not found
The main sequence, a tool for studying human eye movements
- Record: found
- Abstract: found
- Article: not found
Characteristics of two distinct clinical phenotypes in pathologically proven progressive supranuclear palsy: Richardson's syndrome and PSP-parkinsonism.
- Record: found
- Abstract: found
- Article: not found