- Record: found
- Abstract: found
- Article: found
Pharmacokinetics of Ruxolitinib in Patients with Atopic Dermatitis Treated With Ruxolitinib Cream: Data from Phase II and III Studies
Read this article at
Abstract
Background
Pathogenesis of atopic dermatitis (AD) involves the Janus kinase (JAK)/signal transducer and activator of transcription (STAT) pathway. A cream formulation of ruxolitinib, a potent selective JAK1/JAK2 inhibitor, was developed for topical delivery.
Method
Pharmacokinetic data were obtained from three double-blind, vehicle-controlled studies in patients with AD: a phase II study with ruxolitinib cream 0.15%, 0.5%, or 1.5% once daily or 1.5% twice daily (BID), and two phase III studies with 0.75% or 1.5% BID. Effects of baseline characteristics on pharmacokinetics were examined. Correlations were attempted between plasma concentrations and change in hematological parameters over time.
Results
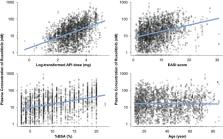
Ruxolitinib plasma concentrations at steady-state ( C ss) increased with cream strength in a less-than-dose-proportional manner. In the phase III studies, overall mean (standard deviation [SD]) C ss after ruxolitinib cream 0.75% and 1.5% BID (23.8 [35.0] and 35.7 [55.0] nM) were a fraction of the half-maximal inhibitory concentration for thrombopoietin-stimulated phosphorylated STAT3 inhibition (281 nM), a JAK/STAT signaling marker. Three covariates were identified for C ss: dose, percent body surface area (%BSA) treated, and baseline Investigator’s Global Assessment score. Mean (SD) bioavailability of ruxolitinib cream 1.5% BID was 6.22% (7.66%). There were no correlations between C ss and any hematological changes except for a transient increase in platelets at week 2.
Related collections
Most cited references53
- Record: found
- Abstract: found
- Article: not found
Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis.
- Record: found
- Abstract: found
- Article: not found
Safety and efficacy of INCB018424, a JAK1 and JAK2 inhibitor, in myelofibrosis.
- Record: found
- Abstract: found
- Article: not found