- Record: found
- Abstract: found
- Article: found
Referral patterns through the lens of health facility readiness to manage obstetric complications: national facility-based results from Ghana
Read this article at
Abstract
Introduction
Countries with high maternal and newborn mortality can benefit from national facility level data that describe intra-facility emergency referral patterns for major obstetric complications. This paper assesses the relationship between referral and facilities’ readiness to treat complications at each level of the health system in Ghana. We also investigate other facility characteristics associated with referral.
Methods
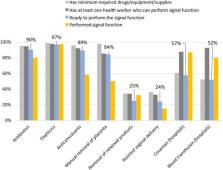
The National Emergency Obstetric and Newborn Care Assessment 2010 provided aggregated information from 977 health facilities. Readiness was defined in a 2-step process: availability of a health worker who could provide life-saving interventions and a minimum package of drugs, supplies, and equipment to perform the interventions. The second step mapped interventions to major obstetric complications. We used descriptive statistics and simple linear regression.
Results
Lower level facilities were likely to refer nearly all women with complications. District hospitals resolved almost two-thirds of all complicated cases, referring 9%. The most prevalent indications for referral were prolonged/obstructed labor and antepartum hemorrhage. Readiness to treat a complication was correlated with a reduction in referral for all complications except uterine rupture. Facility readiness was low: roughly 40% of hospitals and 10% of lower level facilities met the readiness threshold. Facilities referred fewer women when they had higher caseloads, more midwives, better infrastructure, and systems of communication and transport.
Discussion
Understanding how deliveries and obstetric complications are distributed across the health system helps policy makers contextualize decisions about the pathways to providing maternity services. Improving conditions for referral (by increasing access to communication and transport systems) and the management of obstetric complications (increasing readiness) will enhance quality of care and make referral more effective and efficient.
Related collections
Most cited references23
- Record: found
- Abstract: found
- Article: found
Monitoring service delivery for universal health coverage: the Service Availability and Readiness Assessment
- Record: found
- Abstract: found
- Article: found
Bypassing primary care clinics for childbirth: a cross-sectional study in the Pwani region, United Republic of Tanzania
- Record: found
- Abstract: found
- Article: not found