- Record: found
- Abstract: found
- Article: found
The utility of FDG-PET for assessing outcomes in oligometastatic cancer patients treated with stereotactic body radiotherapy: a cohort study
Read this article at
Abstract
Background
Studies suggest that patients with metastases limited in number and destination organ benefit from metastasis-directed therapy. Stereotactic body radiotherapy (SBRT) is commonly used for metastasis directed therapy in this group. However, the characterization of PET response following SBRT is unknown in this population. We analyzed our cohort of patients to describe the PET response following SBRT.
Methods
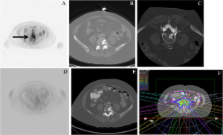
Patients enrolled on a prospective dose escalation trial of SBRT to all known sites of metastatic disease were reviewed to select patients with pre- and post-therapy PET scans. Response to SBRT was characterized on PET imaging based on standard PET response criteria and compared to CT based RECIST criteria for each treated lesion.
Results
31 patients had PET and CT data available before and after treatment for analysis in this study. In total, 58 lesions were treated (19 lung, 11 osseous, 11 nodal, 9 liver, 6 adrenal and 2 soft tissue metastases). Median follow-up was 14 months (range: 3–41). Median time to first post-therapy PET was 1.2 months (range; 0.5-4.1). On initial post-therapy PET evaluation, 96% (56/58) of treated metastases responded to therapy. 60% (35/58) had a complete response (CR) on PET and 36% (21/58) had a partial response (PR). Of 22 patients with stable disease (SD) on initial CT scan, 13 had CR on PET, 8 had PR, and one had SD. Of 21 metastases with PET PR, 38% became CR, 52% remained PR, and 10% had progressive disease on follow-up PET. 10/35 lesions (29%) with an initial PET CR progressed on follow-up PET scan with median time to progression of 4.11 months (range: 2.75-9.56). Higher radiation dose correlated with long-term PET response.
Related collections
Most cited references20
- Record: found
- Abstract: found
- Article: not found
Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases.
- Record: found
- Abstract: found
- Article: not found
Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group.
- Record: found
- Abstract: found
- Article: not found