- Record: found
- Abstract: found
- Article: found
Patterns of Comorbidity and In-Hospital Mortality in Older Patients With COVID-19 Infection
Read this article at
Abstract
Introduction: Older adults are more susceptible to severe COVID-19, with increased all-cause mortality. This has been attributed to their multimorbidity and disability. However, it remains to be established which clinical features of older adults are associated with severe COVID-19 and mortality. This information would aid in an accurate prognosis and appropriate care planning. Here, we aimed to identify the chronic clinical conditions and the comorbidity clusters associated with in-hospital mortality in a cohort of older COVID-19 patients who were admitted to the IRCCS Policlinico San Martino Hospital, Genoa, Italy, between January and April 2020.
Methods: This was a retrospective cohort study including 219 consecutive patients aged 70 years or older and is part of the GECOVID-19 study group. During the study period, upon hospital admission, demographic information (age, sex) and underlying chronic medical conditions (multimorbidity) were recorded from the medical records at the time of COVID-19 diagnosis before any antiviral or antibiotic treatment was administered. The primary outcome measure was in-hospital mortality.
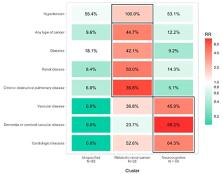
Results: The vast majority of the patients (90%) were >80 years; the mean patient age was 83 ± 6.2 years, and 57.5% were men. Hypertension and cardiovascular disease, along with dementia, cerebrovascular diseases, and vascular diseases were the most prevalent clinical conditions. Multimorbidity was assessed with the Cumulative Illness Rating Scale. The risk of in-hospital mortality due to COVID-19 was higher for males, for older patients, and for patients with dementia or cerebral-vascular disease. We clustered patients into three groups based on their comorbidity pattern: the Metabolic-renal-cancer cluster, the Neurocognitive cluster and the Unspecified cluster. The Neurocognitive and Metabolic-renal-cancer clusters had a higher mortality compared with the Unspecified cluster, independent of age and sex.
Conclusion: We defined patterns of comorbidity that accurately identified older adults who are at higher risk of death from COVID-19. These associations were independent of chronological age, and we suggest that the identification of comorbidity clusters that have a common pathophysiology may aid in the early assessment of COVID-19 patients with frailty to promote timely interventions that, in turn, may result in a significantly improved prognosis.
Related collections
Most cited references20
- Record: found
- Abstract: found
- Article: found
COVID-19: consider cytokine storm syndromes and immunosuppression
- Record: found
- Abstract: found
- Article: not found
Clinical and immunologic features in severe and moderate Coronavirus Disease 2019
- Record: found
- Abstract: found
- Article: not found